Pediatric airway
— what's different.
A pediatric airway is not a small adult airway. Anatomy changes which blade and which view you should expect on attempt #1; physiology changes how much time you have to get there.
Six landmarks differ between children and adults. Each changes a single concrete decision — blade choice, expected view, depth, head position.
-
Tongue
Larger relative to oral cavity. Crowds the view. Externally compressed jaw-thrust and OPA earlier than you would in adults.
-
Epiglottis
Floppy, U-shaped, covers the cords. Use a Miller blade in < 2 yr — lift the epiglottis directly rather than rocking it forward off the vallecula.
-
Vocal cords
Slanted, lower in front.
-
Larynx
Anterior and superior — C3–C4 in infants vs C5–C6 in adults. Expect the cords to appear earlier than they do in adults; BURP only if needed.
-
Cricoid
Functionally narrowest part of the upper airway in young children. Use cuffed ETTs as default (Disma 2024) and pick a size that passes without resistance — don't force.
-
Trachea
Short — ~4 cm in a neonate, ~6 cm at age 1. Right mainstem is easy. Confirm depth at the lip, then bilateral breath sounds.
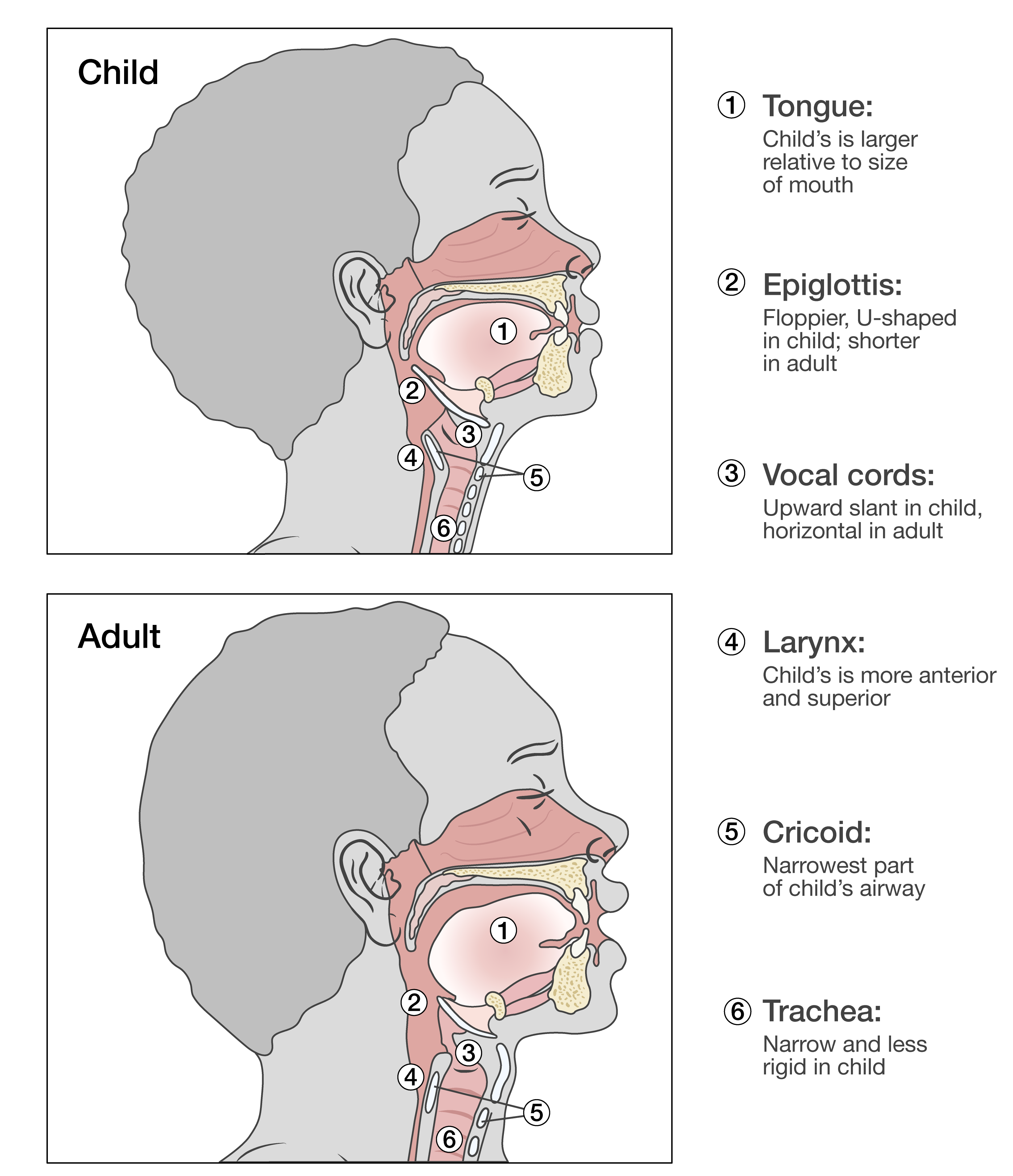 Illustrated — sizing & structure
Illustrated — sizing & structure
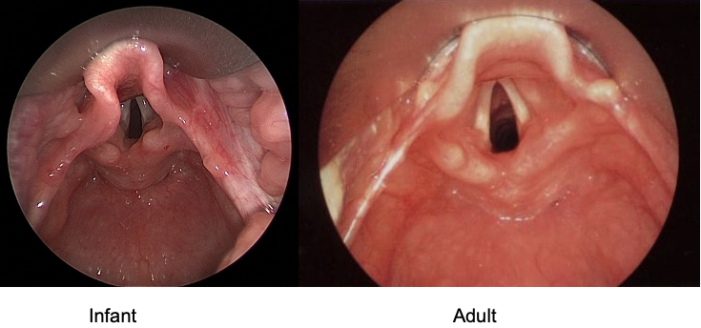 VL view — what you'll see
VL view — what you'll see
Four facts that make every other decision time-critical. They are why pre-oxygenation is non-negotiable, why bradycardia is the warning shot, and why the first attempt has to be the best.
-
O₂ reserve is seconds, not minutes. Oxygen reserve is measured in seconds, not minutes. Infants have higher oxygen consumption per kg and a smaller FRC than adults, so they desaturate faster during apnea. Preoxygenation is essential, apneic oxygenation can help during laryngoscopy, and first-pass optimization matters.
-
Hypoxia → bradycardia, not tachycardia. Hypoxia in infants and young children often causes bradycardia rather than tachycardia. Compared with adults, pediatric patients are more prone to hypoxia-related bradycardia, which is an ominous sign of impending collapse and should prompt immediate oxygenation and ventilation.
-
Cardiac output is rate-dependent. Compared with adults, infants and young children have limited ability to increase stroke volume, so they are more dependent on heart rate to maintain cardiac output. In hypoxia, bradycardia can quickly reduce cardiac output, which lowers cerebral and coronary perfusion and further worsens oxygen delivery.
-
Compliant chest, diaphragm-driven ventilation. Infants have a more compliant chest wall and are more dependent on diaphragmatic breathing, so they fatigue faster under increased work of breathing. During bag-mask ventilation, excessive pressure can cause gastric insufflation, which worsens ventilation and limits chest rise. Squeeze gently and titrate to visible chest rise.
Hypoxia → bradycardia → falling cardiac output → worse perfusion → worse hypoxia.
The window from "looks borderline" to arrest is shorter than the window you trained on in adults. Pre-oxygenate, optimize first attempt, and have BVM/LMA ready to rescue from above before you start.
Each subsequent look in a hypoxic child is more dangerous than the last. The first attempt should be the planned one — best operator, best blade, best position.
Adjunct sizing — memo aid OPA: corner of mouth → angle of mandible. NPA: tip of nostril → tragus. Lubricate; avoid NPA in suspected basilar skull fracture. In an infant who can't be bagged, an NPA is often the difference between "can't BMV" and "can BMV" because young infants are obligate nasal breathers.
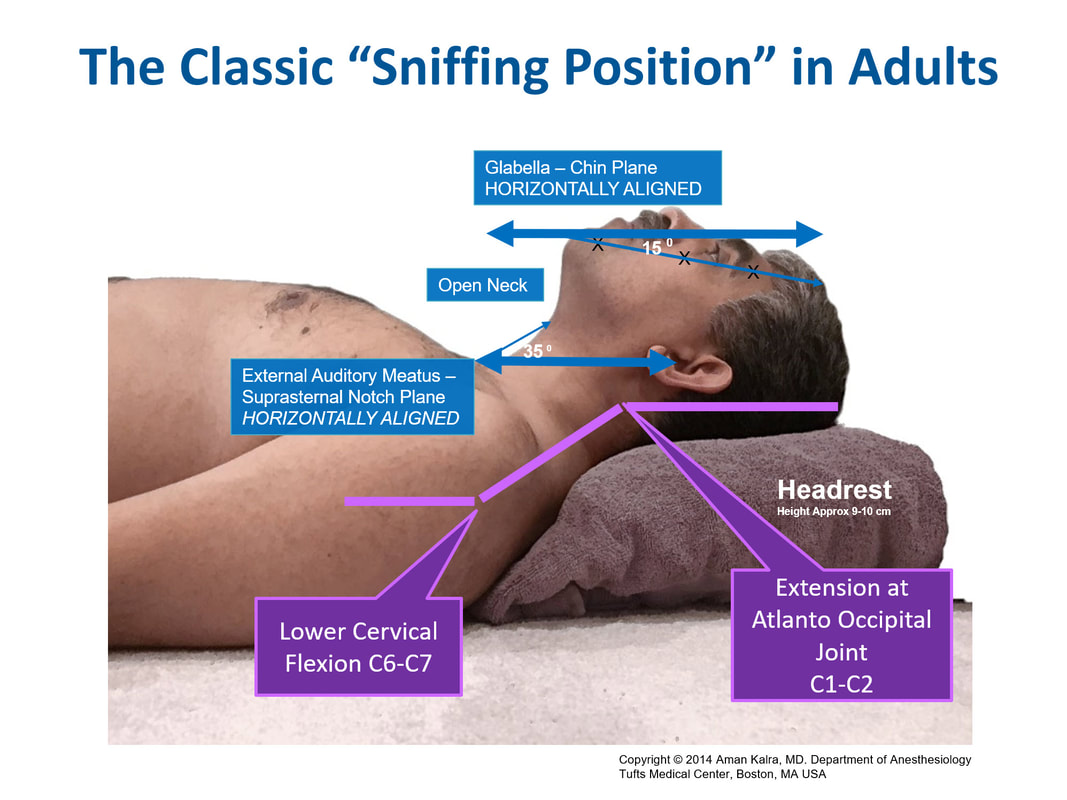 Adult — head elevated
Adult — head elevated
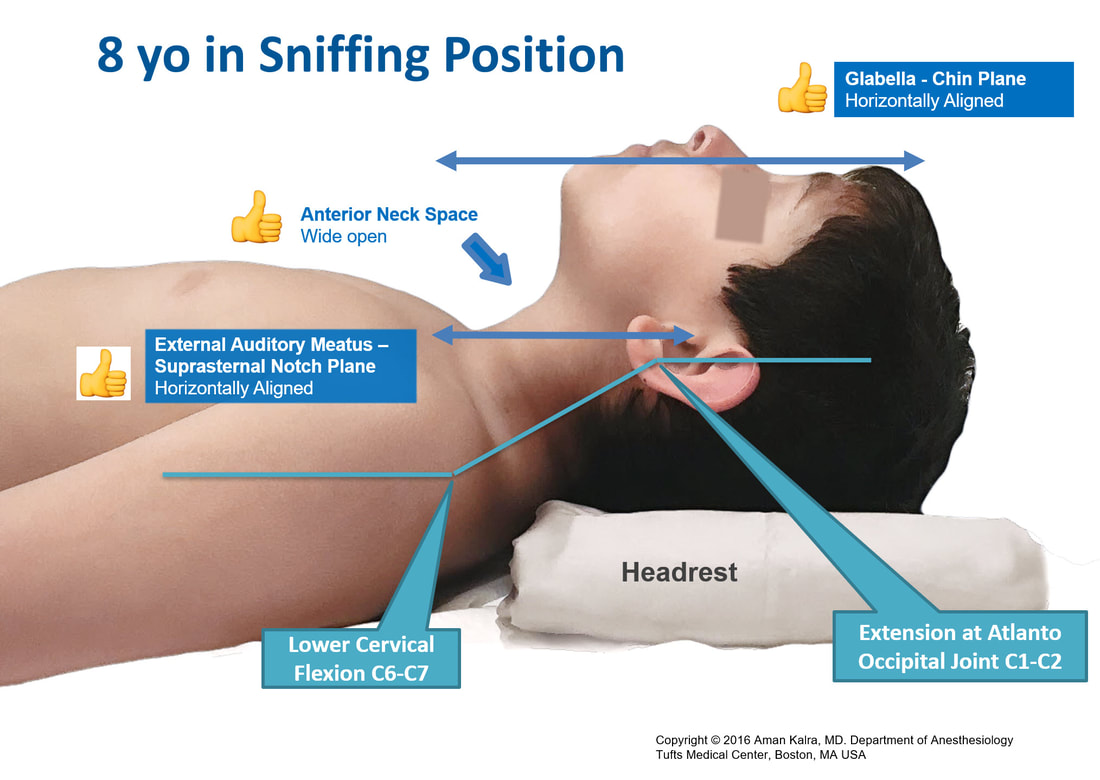 School-age — small pad under occiput
School-age — small pad under occiput
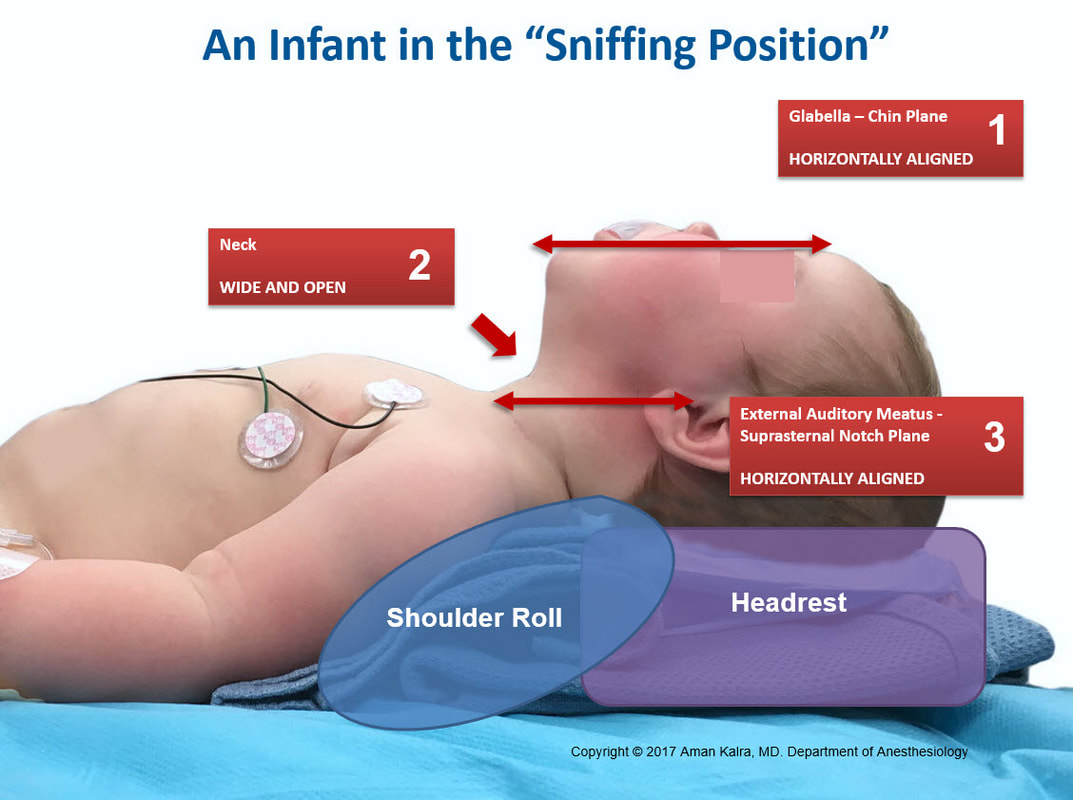 Infant — roll under shoulders
Infant — roll under shoulders
 OPA: mouth → angle of mandible
OPA: mouth → angle of mandible
 NPA: nostril → tragus
NPA: nostril → tragus
Cross-check with Broselow under stress. Use cuffed ETTs as default in all ages including neonates (Disma 2024). Fit, training, and what's stocked matter more than the age label.
| Age | Wt (kg) | ETT cuffed | Depth (cm) | Blade | LMA / i-gel | Bougie | Needle gauge† |
|---|---|---|---|---|---|---|---|
| Neonate | 3 | 3.0–3.5 | 9–10 | Miller 0–1 | 1 | 6F | 14–16G |
| 6 mo | 6 | 3.5 | 11 | Miller 1 | 1.5 | 8F | 14–16G |
| 1 yr | 10 | 4.0 | 12 | Miller 1–1.5 | 1.5 | 10F | 14–16G |
| 2–3 yr | 13 | 4.5 | 13–14 | Mil 1.5 / Mac 2 | 2 | 10F | 14–16G |
| 5 yr | 20 | 5.0 | 15 | Mac 2 | 2 | 10F | 14–16G |
| 8 yr | 25 | 5.5 | 17 | Mac 2–3 | 2.5 | 10–14F | 14G |
| >12 yr | ≥40 | 6.0+ | 18–20 | Mac 3–4 | 3 | 14F | 14G |
CICO reference — can't intubate, can't oxygenate
-
Disma N, et al. Airway management in neonates and infants (ESAIC/BJA). Eur J Anaesthesiol 2024;41:3–23.doi:10.1097/EJA.0000000000001928
-
Black AE, Flynn PER, et al. APA/DAS Paediatric Difficult Airway Guidelines. Paediatr Anaesth 2015;25:346–362.doi:10.1111/pan.12615
-
Fiadjoe JE, et al. PeDI-C registry: pediatric difficult intubation outcomes. Lancet Respir Med 2016;4:37–48.doi:10.1016/S2213-2600(15)00508-1
-
Humphreys S, et al. THRIVE in children (RCT). Br J Anaesth 2017;118:232–238.doi:10.1093/bja/aew401
-
Doctor JR, et al. AIDAA 2025 — Paediatric unanticipated difficult airway. Indian J Anaesth 2025;69:1167–1186.doi:10.4103/ija.ija_1096_25
-
Long E, et al. Endotracheal intubation in the pediatric emergency department. Paediatr Anaesth 2014;24:1204–1211.
-
Mittiga MR, et al. A modern and practical review of RSI in pediatric emergencies. Clin Pediatr Emerg Med 2015;16:172–185.
-
Maskinduction.com. Positioning infants and children for airway management.Visual reference for shoulder-roll and sniffing-position diagrams.