CICO
— can't intubate, can't oxygenate.
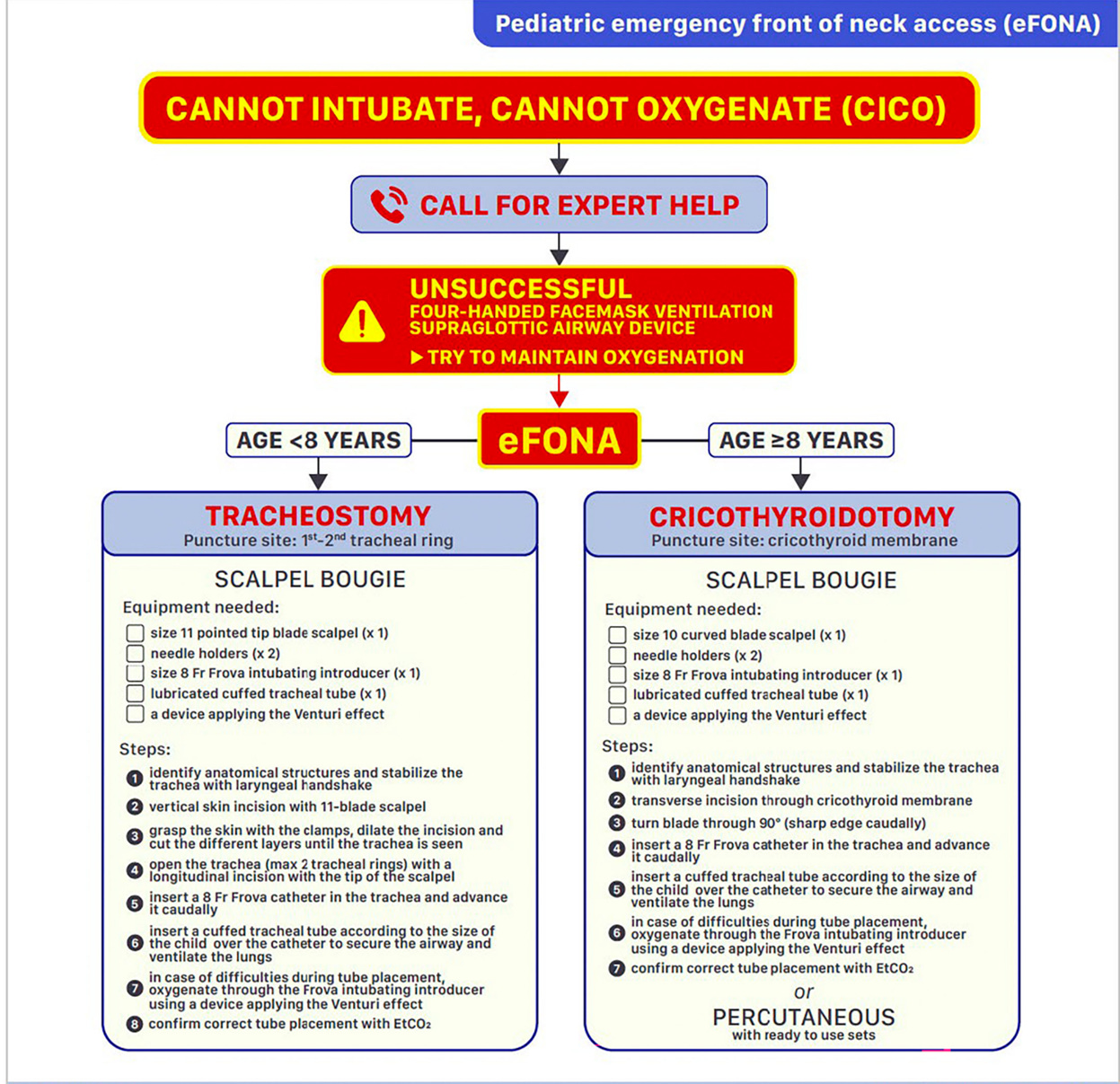
A two-fork algorithm for can't-intubate-can't-oxygenate in children, sized for the kit you actually have, and honest about what the literature can and can't say.
The first decision is anatomic, not by age. The second is which technique your kit and training actually support — name it as a choice and have the other ready as Plan B.
What's true regardless of which pathway you pick.
- A second provider keeps oxygenating from above (BVM / LMA) the entire time.
- Capnography confirms placement. Non-negotiable, both procedures.
- Brief, time-limited attempt — ~45 sec is a useful heuristic, not a validated threshold. If oxygenation isn't establishing, convert.
Both pathways have proponents and shortcomings; neither has high-quality pediatric outcome data. The question to answer in your department before the case: which one are we trained for, and what do we actually have on the wall?
Needle cric + jet ventilation
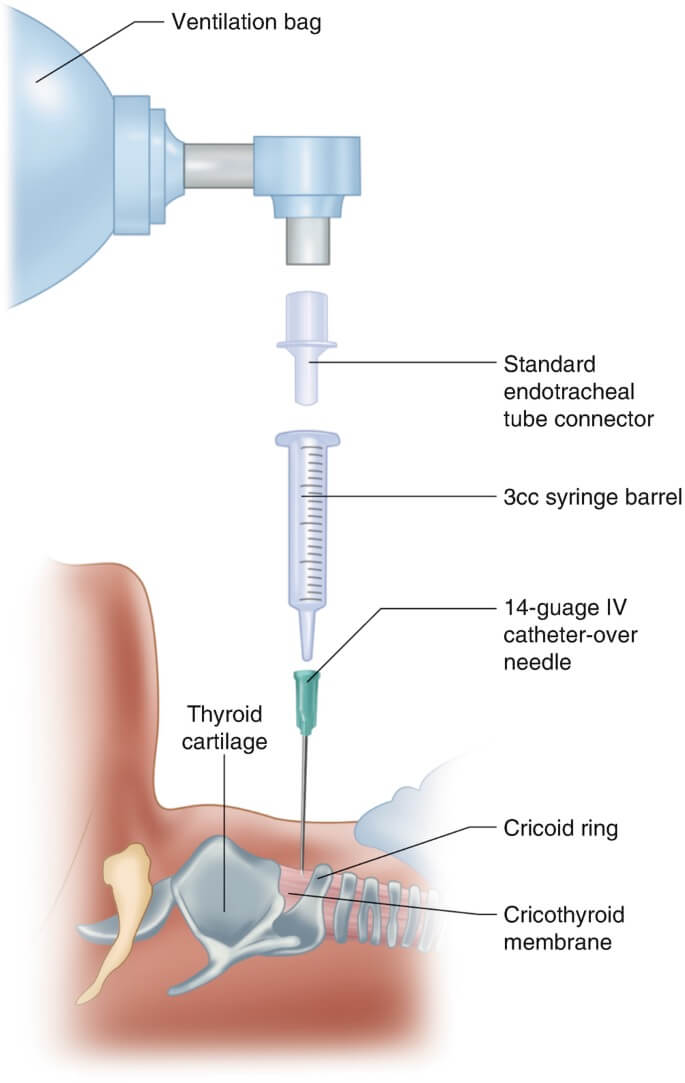
14–16G angiocath through the CTM (largest practical) → connect to a manual jet ventilator (regulated wall O₂) or BVM via a 3.0 ETT adapter (Cole technique). Watch chest rise. Convert if no rise or barotrauma develops. Scalpel reserved for needle failure.
Surgical tracheotomy
Driven by ~50% needle-cric failure in simulation. Vertical midline skin incision below the cricoid → expose trachea → vertical cut through 2 (max 3) tracheal rings → bougie → small ETT. Avoid the lower 25% of the neck (innominate vessels).
A note on the evidence The pediatric CICO literature is small, mostly simulation, and not consistent. Disma 2024 (ESAIC/BJA) and DAS-Paediatric 2015 list the needle-first pathway. Berger-Estilita 2021 and Morgenstern's 2025 First10EM review argue for surgical-first based on needle failure rates in simulation. Both are defensible. What isn't defensible is choosing under time pressure — pick a pathway in advance, drill it, stock for it.
Cole — BVM via a 3.0 ETT adapter — is the realistic default. Knowing what each method actually delivers (and what it doesn't) changes how you set it up.
BVM via 3.0 ETT adapter (Cole technique)
- Pressure
- Limited by BVM peak ~30 cmH₂O (~0.4 PSI)
- Flow
- 100–300 mL delivered per 600 mL squeeze; high resistance through 14–16G
- Use when
- You have a BVM and an ETT adapter — which is everyone
Safer, less barotrauma. Oxygenates; barely ventilates — accept rising CO₂. Watch chest rise; allow long expiration (I:E ≥ 1:4). Hold the catheter manually — it will kink.
Manual jet ventilator (Manujet, ENK, equiv.)
- Pressure
- <5 yr: 5–10 PSI
5–8 yr: 15–25 PSI
>8 yr: 25–50 PSI* - Flow
- High flow per breath; effective tidal delivery
- Use when
- Manual jet ventilator on the wall, training to match
More effective ventilation but real barotrauma risk in kids. Numbers extrapolated from adult / cadaver — not evidence-anchored. Need a patent upper-airway exit (NPA / OPA, retry SGA) or pneumothorax / arrest.
* Pediatric jet pressures Extrapolated from adult work and cadaver setups; treat as starting points, not targets.
Through a 14–16G catheter, the determining variable isn't pressure or volume — it's whether the chest is fully falling between breaths. Operator-controlled, ~1 sec in, 3–5 sec out.
| Step | BVM (Cole) | Manual jet ventilator |
|---|---|---|
| Set | n/a — BVM peak ~30 cmH₂O is fixed | Dial regulator to age-appropriate PSI before connecting |
| Inspiration | Squeeze gently, ~⅓ of 600 mL bag, ~1 sec | Press trigger (Manujet) or occlude side ports (ENK), ~1 sec |
| Expiration | Release. Wait 3–4 sec for passive chest fall | Release / unblock ports. Wait 4–5+ sec |
| I:E ratio | ≥ 1:4 | ≥ 1:4 (longer in smaller children) |
| Watch | Chest rise on squeeze; full chest fall before next squeeze | Chest rise on trigger; full chest fall before next breath |
The 1:4 floor assumes complete upper-airway obstruction — the catheter is the only path in and out. With a patent upper-airway exit (NPA / OPA, retried SGA, jaw-thrust BVM from above), exhalation preferentially follows the native airway and you can ventilate more aggressively — mostly by raising rate, not by squeezing harder. The catheter is flow-limited; harder squeezes mostly raise peak pressure. Chest-fall rule still applies.
Operator timing is the procedure.
Inadequate expiration through a high-resistance catheter → intrathoracic pressure climbs → pneumothorax / arrest. If the chest is not fully falling between breaths, slow down or stop.
First steps — anatomy, physiology, sizing
-
Berger-Estilita J, et al. A primer for pediatric emergency front-of-the-neck access. A&A Pract 2021;15(4):e01444.doi:10.1213/XAA.0000000000001444
-
Morgenstern J. Pediatric front of neck access. First10EM, Apr 2025.Surgical-first argument; reviews failure rates of needle approaches in simulation.
-
Disma N, et al. Airway management in neonates and infants (ESAIC/BJA). Eur J Anaesthesiol 2024;41:3–23.doi:10.1097/EJA.0000000000001928
-
Black AE, Flynn PER, et al. APA/DAS Paediatric Difficult Airway Guidelines. Paediatr Anaesth 2015;25:346–362.doi:10.1111/pan.12615
-
Doctor JR, et al. AIDAA 2025 — Paediatric unanticipated difficult airway. Indian J Anaesth 2025;69:1167–1186.doi:10.4103/ija.ija_1096_25
-
Frerk C, et al. DAS 2015 guidelines — unanticipated difficult intubation in adults. Br J Anaesth 2015;115:827–848.doi:10.1093/bja/aev371
-
Navsa N, Tossel G, Boon JM. Cricothyroid membrane in neonates. Paediatr Anaesth 2005;15:402–406.doi:10.1111/j.1460-9592.2005.01470.x
-
Fiadjoe JE, et al. PeDI-C registry: pediatric difficult intubation outcomes. Lancet Respir Med 2016;4:37–48.doi:10.1016/S2213-2600(15)00508-1
-
Stacey J, et al. Pediatric CICO simulation. Paediatr Anaesth 2012;23:107–113.doi:10.1111/pan.12048
-
Humphreys S, et al. THRIVE in children (RCT). Br J Anaesth 2017;118:232–238.doi:10.1093/bja/aew401
-
Chrimes N. The Vortex approach to CICO. Br J Anaesth 2016;117(Suppl 1):i20–i27.doi:10.1093/bja/aew175
-
EMCrit 184 — Duggan L. Trans-tracheal jet ventilation.